


If you know Dr. Grafinger at all, you probably know that he really enjoys working with exotics; the staff here at TVRH enjoys that he enjoys them. We see hawks and owls and beavers and otters from the wildlife rehabilitator group CLAWS. We work on tigers and lions and caracals and Geoffrey’s cats from the rescue organization The Conservators’ Center (some of their photos are on the wall in his exam room). And recently, some of us got to help out with surgery on a Kemp’s Ridley sea turtle and a green moray eel.
Dr Grafinger has performed surgery on several sea turtles (the previous one from the Karen Beasley Sea Turtle Rescue and Rehabilitation Center, seen here in a previous blog post), so when the North Carolina Aquarium on Roanoke Island needed help with an injured turtle, they gave him a call.

In November of 2014, the Sea Turtle Assistance and Rehabilitation (STAR) Center at the Aquarium obtained a sub-adult Kemp’s Ridley turtle that they nicknamed Finn. Finn had partially healed wounds on his carapace (shell), a puncture wound to the head, and a swollen left front flipper (all possibly inflicted by a boat propeller). The doctor and staff at the aquarium observed that Finn was lethargic, usually kept both eyes closed, and he was not eating.
The wound on the carapace was healing well and required no further treatment. Finn received extensive care for the wound on his head, and bits of bone and necrotic tissue were removed at each cleaning; he was treated with antibiotics, pain medications, and force feedings.
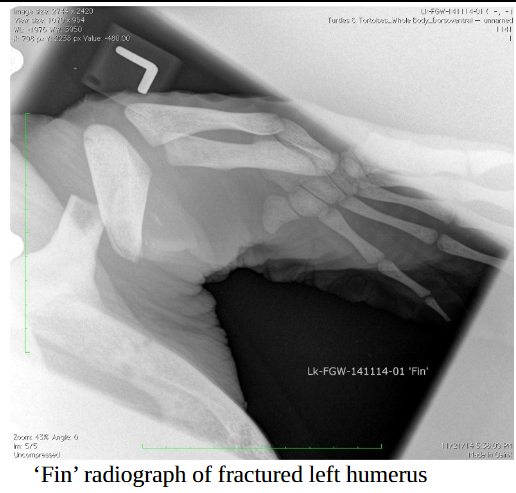
Radiographs and a CT indicated that Finn’s head tilt was probably due to trauma and pain (not brain damage) and that the humerus (the upper “arm” bone of his flipper) was fractured into three pieces, with evidence of bone lysis (the bone was dissolving) as well as possible infection of the bone. This flipper issue was what Dr Grafinger was there to try to fix. Oy!
By the time our TVRH team made the road trip to Manteo, Finn had been undergoing minor procedures and receiving wound care for five months. He was doing some eating on his own and gaining weight, but his neck and flipper wounds were still producing smelly, necrotic material. Dr Grafinger and the aquarium team agreed on a plan of attack, and then it was time to try to repair this amazing animal.

After the experienced aquarium team sedated, intubated, and anesthetized Finn, Dr Grafinger’s surgery assistants (Samantha and Rafe) prepared the site. Dr Grafinger then made the initial incision that would allow him to access the affected area of the humerus without damaging vital nerves or blood flow. What he found added an extra degree of complication to Finn’s surgery – the center piece of bone that had broken loose was dead (the source of the odor and infection).
That dead piece of bone was nearly a third of the length of the humerus, so Dr Grafinger had to find a way to stabilize the remaining bone and reduce that open space. Pins and plates (hardware that’s often used in orthopedic surgeries) just weren’t going to work, so he had to come up with a new plan.
What he used was external fixation. External fixation is a method of stabilizing bone and soft tissue at a distance from the original injury; Dr Grafinger would drill into healthy bone, pass metal pins through those drilled holes, and then pass them back out of the body.
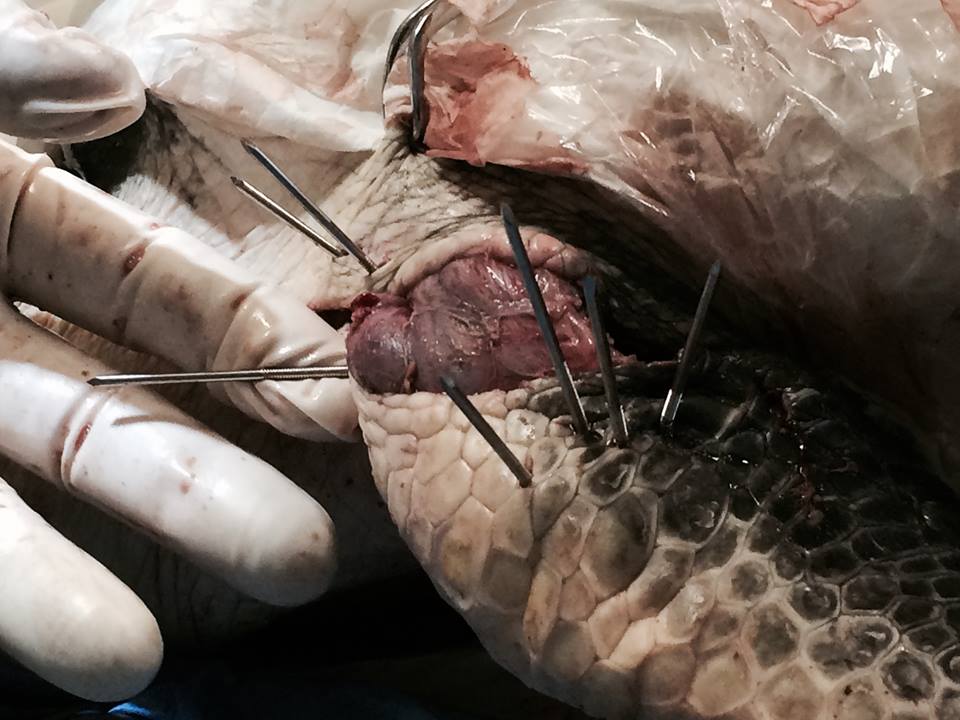

Once the pins were placed to his satisfaction, a fast-hardening epoxy putty was used on the outside of the incision to keep those pins from moving, allowing the bone to heal. Then the entire putty arrangement was protected by using pipe insulation in case Finn managed to bump it in his tank.
Dr Grafinger managed to get those distant bone edges closer together, but Finn will still need to do some significant remodeling (new bone formation) to close that open space. Luckily, the aquarium’s staff veterinarian has found that sea turtles are very good at that sort of repair, so we have high hopes for Finn’s ultimate outcome.
We don’t know yet if Finn will thrive, or even survive; he suffered a lot of damage. But with the support and knowledge of the aquarium team and Dr Grafinger’s best effort to repair that flipper, we’re all hoping that Finn can go back into the wild at some point in the future. You can bet that when that day comes, the TVRH team will be there to see it, cheering him on.






















