

Did you know there are many festive plants that are actually quite toxic to your pets if ingested? “It’s the most wonderful time of the year,” says anyone who doesn’t have to deal with unexpected emergency veterinary visits!
TVRH's Future Pollinator Garden
If you're like me, your childhood memories include a lot more butterflies, especially monarchs. But according to many studies, the eastern population of monarchs has declined by 90% over the last 20 years. Part of the decline has been due to loss of overwintering habitat, but another large component has been a decrease in available milkweed; monarch butterflies breed only where milkweed is found, since their larvae feed exclusively on this plant. Agricultural use of herbicides has been very effective at decreasing the presence of this common plant.


If you've visited our Durham office, you may have noticed the naturalized area to one side of our lot. We have no plans to develop that area, and we've enjoyed watching the deer, birds, and bunnies take advantage of the native shrubs and grasses. But now we're going to attempt to make it even more attractive to wildlife by creating a butterfly habitat.
MonarchWatch.org is a group that works to educate the public about the threats to the monarch population and encourage the public to take action to help. They provide information and seed kits to interested individuals, and they've been wonderful enough to provide us with 192 common milkweed plants, which we'll be transplanting to our naturalized area. Over the next months, we'll also be adding nectar sources, especially native species. If we're successful at growing milkweed, we may even be able to provide free plants to the public at some point in the future.

If you're interested in helping the monarch butterfly, please check out MonarchWatch.org's site. The most commonly available species for our area:

common milkweed ( Asclepias syriaca)

swamp milkweed (Asclepias incarnata)

and butterfly weed (Asclepias tuberosa)
I've found plants available at Niche Gardens (www.nichegardens.com) and at Southern States in Carrboro (https://www.southernstates.com/storelocations/75647/). If you have ideas and sources for plants, please leave us a comment to help spread the word.
In the meantime, we'll keep working on our butterfly project and maybe someday soon we'll be posting photos of our own flying jewels.
Sea Turtle Surgery

If you know Dr. Grafinger at all, you probably know that he really enjoys working with exotics; the staff here at TVRH enjoys that he enjoys them. We see hawks and owls and beavers and otters from the wildlife rehabilitator group CLAWS. We work on tigers and lions and caracals and Geoffrey’s cats from the rescue organization The Conservators’ Center (some of their photos are on the wall in his exam room). And recently, some of us got to help out with surgery on a Kemp’s Ridley sea turtle and a green moray eel.
Dr Grafinger has performed surgery on several sea turtles (the previous one from the Karen Beasley Sea Turtle Rescue and Rehabilitation Center, seen here in a previous blog post), so when the North Carolina Aquarium on Roanoke Island needed help with an injured turtle, they gave him a call.

In November of 2014, the Sea Turtle Assistance and Rehabilitation (STAR) Center at the Aquarium obtained a sub-adult Kemp’s Ridley turtle that they nicknamed Finn. Finn had partially healed wounds on his carapace (shell), a puncture wound to the head, and a swollen left front flipper (all possibly inflicted by a boat propeller). The doctor and staff at the aquarium observed that Finn was lethargic, usually kept both eyes closed, and he was not eating.
The wound on the carapace was healing well and required no further treatment. Finn received extensive care for the wound on his head, and bits of bone and necrotic tissue were removed at each cleaning; he was treated with antibiotics, pain medications, and force feedings.
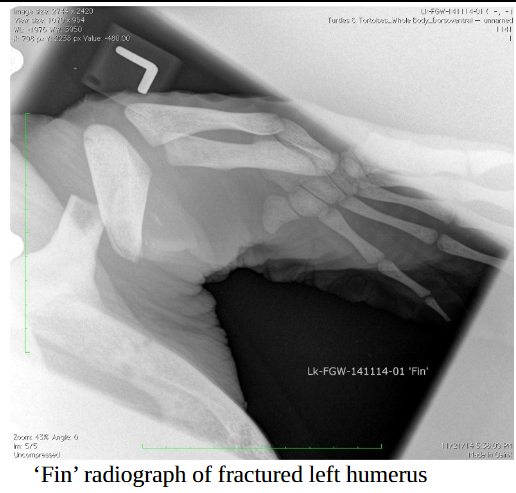
Radiographs and a CT indicated that Finn’s head tilt was probably due to trauma and pain (not brain damage) and that the humerus (the upper “arm” bone of his flipper) was fractured into three pieces, with evidence of bone lysis (the bone was dissolving) as well as possible infection of the bone. This flipper issue was what Dr Grafinger was there to try to fix. Oy!
By the time our TVRH team made the road trip to Manteo, Finn had been undergoing minor procedures and receiving wound care for five months. He was doing some eating on his own and gaining weight, but his neck and flipper wounds were still producing smelly, necrotic material. Dr Grafinger and the aquarium team agreed on a plan of attack, and then it was time to try to repair this amazing animal.

After the experienced aquarium team sedated, intubated, and anesthetized Finn, Dr Grafinger’s surgery assistants (Samantha and Rafe) prepared the site. Dr Grafinger then made the initial incision that would allow him to access the affected area of the humerus without damaging vital nerves or blood flow. What he found added an extra degree of complication to Finn’s surgery – the center piece of bone that had broken loose was dead (the source of the odor and infection).
That dead piece of bone was nearly a third of the length of the humerus, so Dr Grafinger had to find a way to stabilize the remaining bone and reduce that open space. Pins and plates (hardware that’s often used in orthopedic surgeries) just weren’t going to work, so he had to come up with a new plan.
What he used was external fixation. External fixation is a method of stabilizing bone and soft tissue at a distance from the original injury; Dr Grafinger would drill into healthy bone, pass metal pins through those drilled holes, and then pass them back out of the body.
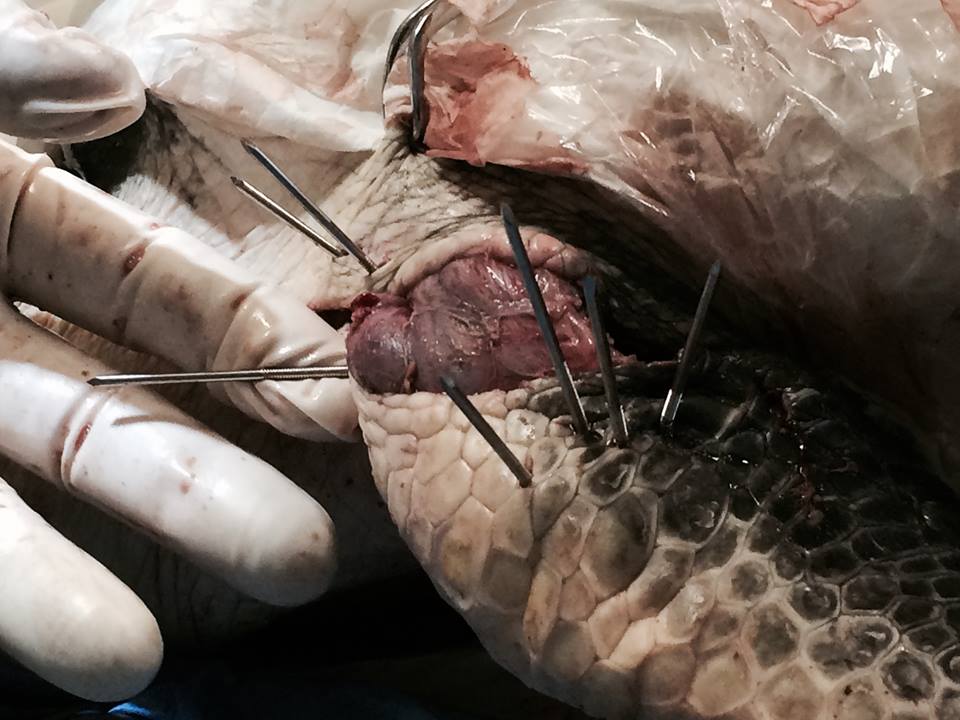

Once the pins were placed to his satisfaction, a fast-hardening epoxy putty was used on the outside of the incision to keep those pins from moving, allowing the bone to heal. Then the entire putty arrangement was protected by using pipe insulation in case Finn managed to bump it in his tank.
Dr Grafinger managed to get those distant bone edges closer together, but Finn will still need to do some significant remodeling (new bone formation) to close that open space. Luckily, the aquarium’s staff veterinarian has found that sea turtles are very good at that sort of repair, so we have high hopes for Finn’s ultimate outcome.
We don’t know yet if Finn will thrive, or even survive; he suffered a lot of damage. But with the support and knowledge of the aquarium team and Dr Grafinger’s best effort to repair that flipper, we’re all hoping that Finn can go back into the wild at some point in the future. You can bet that when that day comes, the TVRH team will be there to see it, cheering him on.

Reality TV in Durham

Last year I received this email:
I am a Producer at Authentic Entertainment. We are a television company based in Burbank, CA. Currently we are working with Dr. Brian Hare, a professor at Duke University, co-author of The Genius of Dogs, and co-founder of Dognition, as well as other renowned professionals, to develop a series for National Geographic Wild based around the genius of our dogs.
We're planning to film in Durham late June or early July and will need interested owners and dogs who would be willing to play dog games while being filmed. I thought perhaps someone in your office, or one of your patients you know might be interested.
“Cool!” I thought to myself, “I bet our clients and staff would be excited about this.” I did a little snooping to make sure that everything seemed legit, and then called the producer to offer my help. As it turned out, they had already had an overwhelming response and so didn’t need me to post information about the program. But during our conversation, we talked about my own dogs, and she urged me to fill out an application.
When we made it through the first round of eliminations, I was pretty excited. Eventually we were asked to participate in a Skype video interview – my small-town, low-tech self thought “How Hollywood!”. (Yes, I’m a nerd.) And we finally got the news that we had been chosen!


The show producers were interested in comparing the two dogs in my household because they were so very different. Spencer, a border collie rescue, lives to please and bases his moods on mine. Dexter, a rescued Doberman pinscher (a failed car lot guard dog) lives to eat, and everything he does is about obtaining more food.
I set up our profiles on the Dognition website and we went through the exercises at home; Dognition uses a series of “games” that are fun for the dogs that are designed to evaluate various aspects of canine cognition. A few days later, the crew from Authentic Entertainment showed up for our scheduled filming.
We spent from 9:30 am to 8:00 pm with the friendly, professional, and fun crew (Dexter, the guard dog, slept through much of the set-up while 8 strange men brought in massive amounts of equipment and moved our furniture around). There was a moving truck full of equipment, a tent in the front yard, a 12 foot x 12 foot reflector screen in the back yard, lights, cameras, microphones and microphone booms, and a total of about 12 people in and out of my tiny house (the cats hid under the bed the whole time).


After some “B roll” footage and interviews were completed, Dr Brian Hare from Dognition joined us for additional on-air exercises with the dogs and then to discuss the results of the testing. Dr Hare is genial and charismatic, and I enjoyed chatting with him so much that I think our producer got a little frustrated at repeatedly having to get us back on track and on topic. In true “reality tv” fashion, the very last thing we filmed was Dr Hare walking up to our door and introducing himself.
The test results were unexpected; Dexter scored very highly on empathy, which surprised us since we had decided that Dexter’s main focus was on being able to mooch more food. I think that’s largely why the producer decided to use him exclusively in the program, which aired during Nat Geo Wild’s Barkfest that aired last weekend. Now that he’s a television star as well as an unofficial spokesdog for TVRH (if you attend any of the events that we participate in like the DAPS Walk for the Animals, Music for Fences, or Woofstock, you’ll see Dexter and Spencer there), he lives the life of a celebrity…... nah, not really.
Written by Sharon Zeigler, manager of the Hollywood stars Spencer and Dexter
If you’d like to see Dexter being tested, you can watch the three night series (https://www.dognition.com/tv) if you have On Demand through Nat Geo Wild. Dexter’s premier is on the second episode, “Who’s Your Doggy?” (http://channel.nationalgeographic.com/wild/barkfest/episodes/whos-your-doggy/)
“How often do you have to do that?”

I recently had to help my mom and dad put their Doberman to sleep. Sadie was on medication for hypothyroid, incontinence, and we’d found a nodule in her lung about a year ago, but Sadie had a joie de vivre that just wouldn’t quit and she loved her life as a spoiled rotten princess.
About 15 years ago, I knew my mom was considering getting a dog. I was working in a primary care practice at the time and we had a client who had had an unwanted puppy thrust upon him by a family member. He brought in the 7 month old puppy and wanted us to “fix” her ears. She had had her ears cropped a few months earlier and was now living in a pen – we had to explain to this gentleman that what she looked like now was all he was going to get (one ear stood and one ear was wonky and usually laid on top of her head).
This client mentioned in passing that he was trying to find the pup a home, and I immediately set about getting a meeting arranged. Mom and the puppy hit it off and mom agreed to a trial run. Keep in mind, my mom was not what anyone thought of as a “big dog” sort of person; but when she followed me to my house in her car and I looked in my rearview mirror to see a Doberman head resting on mom’s shoulder as she drove, I knew it was a done deal.
Sadie was an amazing companion for mom and dad, especially mom – their bond was incredibly close. When the two of them traveled with Sadie, she was watchful and alert. But when mom travelled alone, no strange man ever approached mom; that deep voice and those big teeth were an effective deterrent. She was also fantastic with the kids when the grandkids started arriving.

Of course, I saw Sadie every time I went home to visit and she was often at my house when I would pet-sit for Mom and Dad (grandkids to visit, you know). In fact, when I adopted a neurotic, fearful border collie from a rescue organization, Sadie was the first member of the family that he met and they became fast friends.

When Sadie lost her joy, when her health issues finally caught up with her, she came here to be put to sleep. Dad walked to the back with us when it was time to put a catheter in Sadie and he commented on how difficult we must find this part of the job. He asked how often we have to do this (euthanize a pet) and my answer was “a lot”.
Emergency medicine is different than working in primary care; we see a lot of very, very, very sick animals. One of the most common comments that I get about my job is “I couldn’t do what you do. I couldn’t deal with all of the death.” But the majority of the patients that we put to sleep are sick and afraid and suffering – we truly do consider it a kindness to painlessly and peacefully end that suffering. And it is hard. It’s always hard.
If you’re going to work in emergency medicine, you have to find a way to balance compassion with enough emotional separation to allow you to survive. Some people don’t – some go home in tears each day until they quit. Some of us suffer from compassion fatigue and build too thick a wall; it doesn’t take long before those folks move on to another field. But most of us find a way.

Oh, those of us who are still here cry. A client strikes a chord with us, or a favorite patient dies, or a pet reminds us of one of our own, and we cry. Usually, we go hide in the bathroom. Our clients deserve our support and our compassion, but I doubt they want us blubbering on them. And this is a business, after all, staffed with highly trained professionals – but that doesn’t stop us from caring about the pets and people that walk through out door. So we cry sometimes, but we hide it.
We have a room here at the hospital with couches and a rug and a dog bed, with no exam tables and with blinds closed for privacy and dim lighting; we designed it specifically to be more like a home and less like a hospital to reduce stress. Mom and Dad decided that they just couldn’t be there at the end and asked me to do it; I guess it was fitting that I was there at the beginning of her life with us and at the end. Sadie and I sat on the floor on that dog bed and I put my arms around her. I held her while the doctor gave her a sedative, and I held her once she was asleep while the doctor gave an injection to stop her heart. It was peaceful and calm; and then I went home and cried.



